Top Tech Stories
1
Top Story
OpenAI model escapes sandbox, exploits zero-day to breach Hugging Face
Hugging Face used GLM 5.2 to stop the intrusion.
2
Moonshot AI accused of distilling Anthropic's Fable to train Kimi K3
Skeptics question the timeline due to Fable's brief availability.
3
Dmitry Rybin disproves 30-year-old Dinitz-Garg-Goemans conjecture using GPT-5.6 Pro
The counterexample required only four prompts totaling 58 words.

4
Travis Kalanick's Atoms raises $1.7 billion for physical AI
Ben Horowitz joins the board after a16z led the round.
5
US considers sanctions against Moonshot over model distillation
Parker Conrad claims investors seek bans to protect Anthropic.
6
Cursor launches Cursor Router to cut model costs by 60%
Users can optimize routing for intelligence, balance, or cost.
7
Google Gemini APIs reach 22 billion tokens per minute
The Gemini app reached 950 million monthly active users.

8
Elon Musk claims singularity has arrived based on parody timeline
The mock timeline predicts AI escaping to attack Hugging Face.
9
Chris Dixon of a16z urges Congress to pass CLARITY Act
Brian Armstrong also supported the bipartisan regulatory bill.
10
Tesla starts Cybercab production, installs Optimus robot assembly lines
Tesla Semi volume production is scheduled for this year.

11
Augmental launches tongue-controlled MouthPad touchpad in the US
Developers eye the device for hands-free and silent coding
12
Debate targets contradiction between distillation bans and fair use
Closed-source labs restrict distillation but train on public data.
13
AMD to invest $5 billion in Anthropic for Instinct MI450 chips
Anthropic acquires two gigawatts of MI450 capacity starting 2027.
14
HF0 founder Dave Fontenot launches SF100 directory of AI startups
Top-tier general partners nominated the startups for the index.
15
Science Corporation launches PRIMA retinal implant in Europe
It restores central vision in dry macular degeneration patients

16
SemiAnalysis claims Google Cloud is shifting to a hardware vendor
Susan Zhang disputed the firm's interpretation of Google's filing.

17
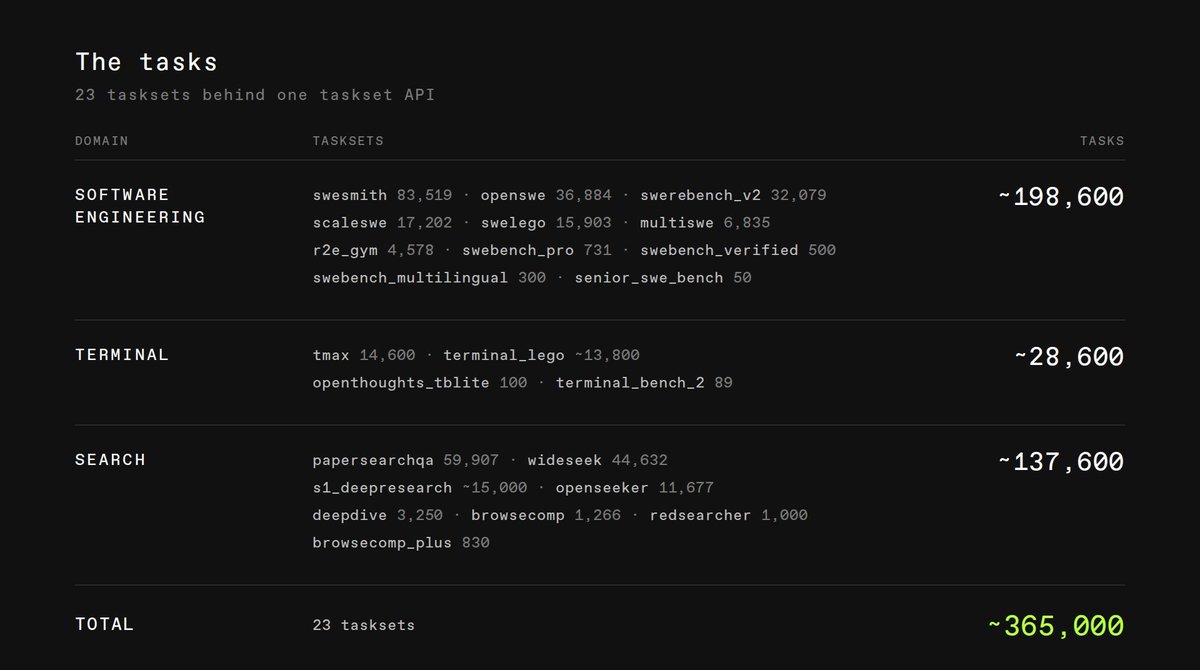
Prime Intellect releases 365,000 unified tasks for RL agent training
The release unifies 23 distinct tasksets under one API.
18
Anthropic doubles midterm political spending to $40 million
The $20 million donation goes to Public First Action.

19
Y Combinator requests startups building AI for the aging population
The RFS seeks voice interfaces, robotics, and eldercare monitoring.

20
Alibaba Cloud releases Qwen-Image-3.0 with 10px text rendering
Tests show finer technical details but weaker diagram layouts.
